Pulmonary artery sarcoma (PAS) is an extremely rare and aggressive malignancy, often misdiagnosed as pulmonary thromboembolism due to overlapping clinical presentations. This case report describes a 35-year-old female with progressive dyspnea and syncope, initially managed as pulmonary embolism. Despite anticoagulation therapy, persistent intracardiac masses were identified, prompting urgent surgical intervention. Transesophageal echocardiography (TEE) played a pivotal role intraoperatively, revealing a large mobile mass obstructing the pulmonary artery and causing hemodynamic instability. Following cardiac arrest, emergency surgery with extracorporeal circulation support was performed. Postoperative TEE demonstrated reduced mass size and improved pulmonary blood flow, although histopathological examination confirmed malignant carcinosarcoma. Unfortunately, the patient experienced recurrent syncopal episodes post-discharge and succumbed to the illness despite resuscitation efforts. This case highlights the diagnostic challenges of PAS and the indispensable role of TEE throughout the perioperative period. TEE provides real-time hemodynamic monitoring, precise tumor localization, and assessment of right ventricular function, facilitating timely surgical decisions. Intraoperatively, TEE continuously monitors for sudden hemodynamic changes, such as right ventricular outflow tract obstruction, and guides therapeutic interventions. Postoperatively, TEE aids in evaluating surgical outcomes, detecting residual masses or complications, and informing postoperative management strategies. Multi-planar TEE assessment, especially the ME gastric view, is crucial for comprehensive evaluation. This case underscores the importance of integrating TEE into the management of PAS to optimize patient outcomes.
| Published in | International Journal of Anesthesia and Clinical Medicine (Volume 13, Issue 2) |
| DOI | 10.11648/j.ijacm.20251302.16 |
| Page(s) | 93-97 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Pulmonary Artery Sarcoma, Pulmonary Embolism, Transesophageal Echocardiography, Misdiagnosis, Multidisciplinary Management
PAS | Pulmonary Artery Sarcoma |
TTE | Transthoracic Echocardiography |
CTPA | Computed Tomography Pulmonary Angiography |
PE | Pulmonary Embolism |
TEE | Transesophageal Echocardiography |
ICU | Intensive Care Unit |
POD | Postoperative Day |
RVOT | Right Ventricular Outflow Tract |
CMR | Cardiac Magnetic Resonance |
CT | Computed Tomography |
TV | Tricuspid Valve |
PA | Pulmonary Artery |
RV | Right Ventricular |
| [1] | Bai, X., & Ruan, L. A case report of primary pulmonary artery intimal sarcoma. European journal of medical research. 2021, 26(1), 89. |
| [2] | Kronzer, E., Robinson, S. I., Collins, D. A., & McBane, R. D., 2nd. Primary pulmonary artery sarcoma versus pulmonary thromboembolism: a multimodal imaging comparison. Journal of thrombosis and thrombolysis, 2021, 52(4), 1129-1132. |
| [3] | Rali, P. M., & Criner, G. J. Submassive Pulmonary Embolism. American journal of respiratory and critical care medicine. 2018, 198(5), 588-598. |
| [4] | Nguyen, P. C., Stevens, H., Peter, K., & McFadyen, J. D. (2021). Submissive Pulmonary Embolism: Current Perspectives and Future Directions. Journal of clinical medicine. 2021, 10(15), 3383. |
| [5] | Kahn, S. R., & de Wit, K. Pulmonary Embolism. The New England journal of medicine. 2022, 387(1), 45-57. |
| [6] | N Mercken, K., Sneyers, V., & Di Dedda, E. (2024). Pulmonary Artery Intimal Sarcoma. Journal of the Belgian Society of Radiology. 2024, 108(1), 105. |
| [7] | Xiao, Q., Li, X., Li, Y., Wu, Z., Xu, C., Chen, Z., & He, W.. Biological drug and drug delivery-mediated immunotherapy. Acta pharmaceutica Sinica. 2021, B, 11(4), 941-960. |
| [8] | Zhao, M., Nie, P., Guo, Y., & Chen, H. Pulmonary artery intimal sarcoma: A rare cause of filling defects in pulmonary arteries. The American journal of the medical sciences. 2022, 364(5), 655-660. |
| [9] | de Groot, M. R., van Marwijk Kooy, M., Pouwels, J. G., Engelage, A. H., Kuipers, B. F., & Büller, H. R. The use of a rapid D-dimer blood test in the diagnostic work-up for pulmonary embolism: a management study. Thrombosis and haemostasis. 1999, 82(6), 1588-1592. |
| [10] | Assi, T., Kattan, J., Rassy, E., Moussa, T., Nassereddine, H., Honore, C., Adam, J., Terrier, P., Dumont, S., Mir, O., & Le Cesne, A. A comprehensive review on the diagnosis and management of intimal sarcoma of the pulmonary artery. Critical reviews in oncology/hematology. 2020, 147, 102889. |
| [11] | Wyler von Ballmoos, M. C., Chan, E. Y., & Reardon, M. J. Imaging and Surgical Treatment of Primary Pulmonary Artery Sarcoma. The international journal of cardiovascular imaging. 2019, 35(8), 1429-1433. |
| [12] | Nicoara, A., Skubas, N., Ad, N., Finley, A., Hahn, R. T., Mahmood, F., Mankad, S., Nyman, C. B., Pagani, F., Porter, T. R., Rehfeldt, K., Stone, M., Taylor, B., Vegas, A., Zimmerman, K. G., Zoghbi, W. A., & Swaminathan, M. Guidelines for the Use of Transesophageal Echocardiography to Assist with Surgical Decision-Making in the Operating Room: A Surgery-Based Approach: From the American Society of Echocardiography in Collaboration with the Society of Cardiovascular Anesthesiologists and the Society of Thoracic Surgeons. Journal of the American Society of Echocardiography: official publication of the American Society of Echocardiography. 2020, 33(6), 692-734. |
| [13] | Assaf, Yazan., Nasser, Maher., Nasser, Maher., Nasser, Maher., & Nasser, Maher. Pulmonary Embolism Following Incomplete Surgical Resection of a Right Ventricular Myxoma: A Case Report and Review of the Literature. Cardiology and therapy. 2018, 7(1), 107-117. |
| [14] | Chan, E. Y., Ravi, V., Ali, A., Nguyen, D. T., Graviss, E. A., MacGillivray, T. E., & Reardon, M. J. Surgical Management of Primary Pulmonary Artery Sarcoma. Seminars in thoracic and cardiovascular surgery. 2023, 35(1), 53-64. |
| [15] | Alizadehasl, A., Najdaghi, S., Mohseni Salehi, M., Meshgi, S., Hosseini Jebelli, S. F., Yalameh Aliabadi, A., Hakimian, H., Forati, S., Safavirad, A., & Narimani Davani, D. A Comprehensive Insight Into Primary Intimal Sarcoma of the Pulmonary Artery; From Diagnosis to Management: A Case Report and Review of the Literature. Clinical case reports. 2024, 12(11), e9580. |
APA Style
Chen, Y., Jing, Y. (2025). Application of Perioperative Transesophageal Echocardiography in Resection of Pulmonary Artery Sarcoma: A Case Report. International Journal of Anesthesia and Clinical Medicine, 13(2), 93-97. https://doi.org/10.11648/j.ijacm.20251302.16
ACS Style
Chen, Y.; Jing, Y. Application of Perioperative Transesophageal Echocardiography in Resection of Pulmonary Artery Sarcoma: A Case Report. Int. J. Anesth. Clin. Med. 2025, 13(2), 93-97. doi: 10.11648/j.ijacm.20251302.16
@article{10.11648/j.ijacm.20251302.16,
author = {Yang Chen and Yang Jing},
title = {Application of Perioperative Transesophageal Echocardiography in Resection of Pulmonary Artery Sarcoma: A Case Report
},
journal = {International Journal of Anesthesia and Clinical Medicine},
volume = {13},
number = {2},
pages = {93-97},
doi = {10.11648/j.ijacm.20251302.16},
url = {https://doi.org/10.11648/j.ijacm.20251302.16},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijacm.20251302.16},
abstract = {Pulmonary artery sarcoma (PAS) is an extremely rare and aggressive malignancy, often misdiagnosed as pulmonary thromboembolism due to overlapping clinical presentations. This case report describes a 35-year-old female with progressive dyspnea and syncope, initially managed as pulmonary embolism. Despite anticoagulation therapy, persistent intracardiac masses were identified, prompting urgent surgical intervention. Transesophageal echocardiography (TEE) played a pivotal role intraoperatively, revealing a large mobile mass obstructing the pulmonary artery and causing hemodynamic instability. Following cardiac arrest, emergency surgery with extracorporeal circulation support was performed. Postoperative TEE demonstrated reduced mass size and improved pulmonary blood flow, although histopathological examination confirmed malignant carcinosarcoma. Unfortunately, the patient experienced recurrent syncopal episodes post-discharge and succumbed to the illness despite resuscitation efforts. This case highlights the diagnostic challenges of PAS and the indispensable role of TEE throughout the perioperative period. TEE provides real-time hemodynamic monitoring, precise tumor localization, and assessment of right ventricular function, facilitating timely surgical decisions. Intraoperatively, TEE continuously monitors for sudden hemodynamic changes, such as right ventricular outflow tract obstruction, and guides therapeutic interventions. Postoperatively, TEE aids in evaluating surgical outcomes, detecting residual masses or complications, and informing postoperative management strategies. Multi-planar TEE assessment, especially the ME gastric view, is crucial for comprehensive evaluation. This case underscores the importance of integrating TEE into the management of PAS to optimize patient outcomes.},
year = {2025}
}
TY - JOUR T1 - Application of Perioperative Transesophageal Echocardiography in Resection of Pulmonary Artery Sarcoma: A Case Report AU - Yang Chen AU - Yang Jing Y1 - 2025/08/18 PY - 2025 N1 - https://doi.org/10.11648/j.ijacm.20251302.16 DO - 10.11648/j.ijacm.20251302.16 T2 - International Journal of Anesthesia and Clinical Medicine JF - International Journal of Anesthesia and Clinical Medicine JO - International Journal of Anesthesia and Clinical Medicine SP - 93 EP - 97 PB - Science Publishing Group SN - 2997-2698 UR - https://doi.org/10.11648/j.ijacm.20251302.16 AB - Pulmonary artery sarcoma (PAS) is an extremely rare and aggressive malignancy, often misdiagnosed as pulmonary thromboembolism due to overlapping clinical presentations. This case report describes a 35-year-old female with progressive dyspnea and syncope, initially managed as pulmonary embolism. Despite anticoagulation therapy, persistent intracardiac masses were identified, prompting urgent surgical intervention. Transesophageal echocardiography (TEE) played a pivotal role intraoperatively, revealing a large mobile mass obstructing the pulmonary artery and causing hemodynamic instability. Following cardiac arrest, emergency surgery with extracorporeal circulation support was performed. Postoperative TEE demonstrated reduced mass size and improved pulmonary blood flow, although histopathological examination confirmed malignant carcinosarcoma. Unfortunately, the patient experienced recurrent syncopal episodes post-discharge and succumbed to the illness despite resuscitation efforts. This case highlights the diagnostic challenges of PAS and the indispensable role of TEE throughout the perioperative period. TEE provides real-time hemodynamic monitoring, precise tumor localization, and assessment of right ventricular function, facilitating timely surgical decisions. Intraoperatively, TEE continuously monitors for sudden hemodynamic changes, such as right ventricular outflow tract obstruction, and guides therapeutic interventions. Postoperatively, TEE aids in evaluating surgical outcomes, detecting residual masses or complications, and informing postoperative management strategies. Multi-planar TEE assessment, especially the ME gastric view, is crucial for comprehensive evaluation. This case underscores the importance of integrating TEE into the management of PAS to optimize patient outcomes. VL - 13 IS - 2 ER -
Country Department of Anesthesiology, West China Hospital Sichuan University, Chengdu, China
Biography: Yang Chen is an anesthesiologist working at West China Hospital of Sichuan University. In 2024, she obtained a master's degree in anesthesiology from West China Hospital of Sichuan University. The main research direction is perioperative analgesia.
Research Fields: perioperative analgesia, regional anesthesia, nerve block anesthesia, pain, anesthesia management, orthopedic surgery management

Country Department of Anesthesiology, West China Hospital Sichuan University, Chengdu, China
Research Fields: perioperative analgesia, regional anesthesia, nerve block anesthesia, pain, anesthesia management, orthopedic surgery management
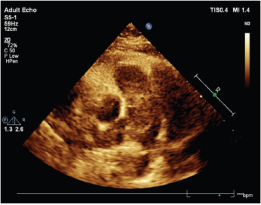
Figure 1. Preoperative TTE (a giant mass in the main pulmonary artery trunk).
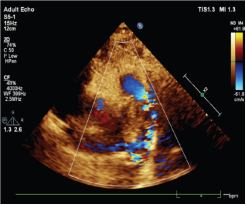
Figure 2. TTE (blood flow through the main pulmonary artery was difficult).
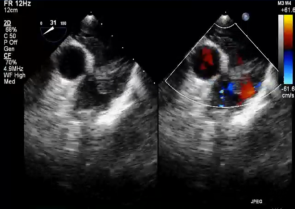
Figure 3. Preoperative TEE (a giant mass in the main pulmonary artery trunk. And blood flow through the main pulmonary artery was difficult.).
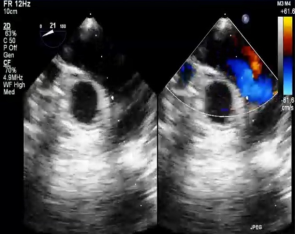
Figure 4. Postoperative TEE (The mass was smaller and pulmonary arterial blood flow had increased compared to before the operation).

