Epiglottic masses may present as cystic, infectious, neoplastic, or systemic disease manifestations. Their size and location can lead to airway obstruction, increasing the difficulty of general anesthesia induction. Perioperative management for such patients requires meticulous planning to prevent sudden airway challenges post-anesthesia. Multidisciplinary collaboration (anesthesiology and otolaryngology) and the use of visualization devices (e.g., video laryngoscopy) are critical for ensuring airway safety. We described the anesthesia management for a 69-year-old male with a glottic mass. Laryngoscopy and CT revealed a 2.7×2.0 cm cauliflower-like mass on the lingual surface of the epiglottis (squamous high-grade intraepithelial neoplasia/carcinoma in situ). After comprehensive evaluation of the airway and perioperative drug interactions, appropriate sedatives, analgesics, and muscle relaxants were selected. The patient successfully completed the surgery and was discharged. The selection of the anesthesia intubation approach for epiglottic masses should be predicated on the size and location of the masses, along with the patient's specific circumstances. This case underscores the significance that conducting a thorough preoperative assessment of the patient prior to surgery and implementing multidisciplinary cooperation in light of the patient's condition can substantially mitigate anesthesia - related risks. Video laryngoscopy-assisted endotracheal intubation is the preferred method for protecting lingual epiglottic masses, minimizing tumor injury risks. However, its successful and safe implementation requires collaboration between experienced anesthesiology and otolaryngology teams.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Epiglottic masses can be manifestations of cystic, granulomatous, infectious, neoplastic, or systemic conditions. They vary in size and may be solitary or multiple
[1]
Matsumoto T, Iwamoto T, Nakajima Y, et al. Evaluation of the Adequacy of Using the Supraglottic Airway Device (i-gel®) in Cases With Epiglottic Masses: A Mannequin Simulation Study [J]. Cureus, 2024, 16(11): e74734.
. Symptomatic epiglottic masses or those causing airway obstruction may require surgical resection
[2]
Varathan V, Mat Baki M, Kalimuthu S. A Case Report of an Unusual Presentation of Epiglottic Cyst Causing Airway Obstruction in an Adult [J]. Cureus, 2023, 15(3): e35863.
. The presence of epiglottic masses may occasionally interfere with laryngoscope insertion into the airway, potentially impeding the induction of general anesthesia
[3]
Zhang R, Jiang X, Feng J. Difficult endotracheal intubation due to a large epiglottic cyst: A case report [J]. Medicine (Baltimore), 2023, 102(24): e34026.
. In such patients, even with mild clinical symptoms, perioperative planning should be meticulously conducted to prevent significant airway obstruction—which may present rapidly following administration of sedatives and induction agents—from precipitating difficult airway scenarios
[5]
Takaishi K, Otsuka R, Fujiwara S J, et al. A Retrospective Case Series of Anesthetic Patients With Epiglottic Cysts [J]. Anesth Prog, 2021, 68(3): 168-177.
. Therefore, anesthesiologists may encounter unforeseen ventilation challenges.
In this case, we report a case of a male patient with an epiglottic mass who underwent difficult tracheal intubation due to the lesion's location and dimensions. Our findings indicate that before handling patients undergoing throat surgery, it is crucial to carefully assess the location and size of the lesion, check for concurrent airway difficulties, and select the appropriate visual equipment for anesthesia induction accordingly.
2. Case Presentation
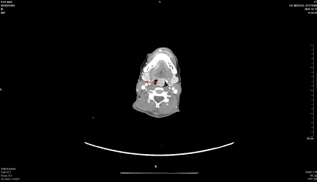
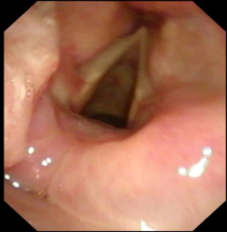
A 69-year-old male patient presented to our institution with pharyngeal pain. Laryngoscopic examination revealed an exophytic lesion on the lingual surface of the epiglottis (Figure 1), with pathological analysis establishing high-grade squamous intraepithelial neoplasia /carcinoma in situ. Preoperative computed tomography (CT) of the patient demonstrated markedly irregular soft tissue thickening involving the epiglottis, predominantly affecting its left portion where a mass-like lesion measuring approximately 2.7 × 2.0 cm in cross-section was observed. The lesion exhibited heterogeneous intense enhancement on contrast-enhanced imaging, extending to involve the epiglottic vallecula and left aryepiglottic fold (Figure 2). Thus, the patient was scheduled for surgical resection under general anesthesia.
The day prior to surgery, following the pre-anesthetic evaluation, the responsible anesthesiologist conducted an initial airway assessment. The patient exhibited a Mallampati class II view with visualization of the soft palate, fauces, and partial uvula. Cervical spine mobility was unrestricted. Bedside questioning confirmed absence of snoring or awakening from breathlessness, with no positional dyspnea during sleep.
After formulating an airway management strategy based on CT and laryngoscopic imaging, the anesthesiologist engaged in multidisciplinary deliberation with ENT surgeons regarding airway protection. Given the optimal glottic exposure demonstrated by video laryngoscopy (Figure 3), the decision was made to proceed with rapid sequence induction followed by orotracheal intubation after confirming adequate spontaneous ventilation. Contingency protocols were established as follows:
Primary backup: Fiberoptic bronchoscope-assisted orotracheal intubation, Secondary backup: Two ENT surgeons present from induction onset, prepared for emergent intervention, Tertiary measure: Surgical airway readiness with tracheostomy tray immediately available.
Upon the patient's arrival in the operating room, standard perioperative monitoring was established, including electrocardiography, pulse oximetry, non-invasive blood pressure, end-tidal carbon dioxide monitoring, and peripheral intravenous access. Following adequate preoxygenation via facemask, we induced anesthesia while preserving spontaneous respiration using Sufentanil 0.1 μg/kg and Propofol 1 mg/kg. After loss of consciousness, uneventful facemask ventilation was initiated using the anesthesia machine ventilator, followed by administration of Rocuronium 1 mg/kg based on ideal body weight.
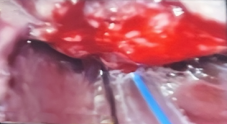
Two minutes later, the anesthesiologist performed orotracheal intubation using video laryngoscopy. Under direct visualization, a cauliflower-like tumor mass was observed on the lingual surface of the epiglottis (Figure 4). The anesthesiologist meticulously administered topical anesthesia to the glottis and periglottal mucosa via a spray catheter with 2% lidocaine, deliberately avoiding the tumor to prevent post-extubation complications including hemorrhage or laryngospasm triggered by coughing. A 7.0-mm reinforced endotracheal tube was then advanced through the glottis (Figure 5). Following intubation, anesthesia maintenance was achieved with 2.5% end-tidal sevoflurane and remifentanil infusion at 0.15 μg/kg/min. The anesthetic and surgical course proceeded without incident.
The operation lasted for 131 minutes. After the tumor was completely removed, the surgeon performed a tracheotomy on the patient. The patient was transferred to the post-anesthesia care unit (PACU) for recovery. After 30 minutes of continuous monitoring, the Aldrete score reached 9/10, prompting transfer to the general ward. The patient was discharged uneventfully on the 11th day postoperatively.
Figure 2. The lesion exhibited heterogeneous intense enhancement on contrast-enhanced imaging, extending to involve the epiglottic vallecula and left aryepiglottic fold.
Figure 4. The anesthesiologist performed orotracheal intubation using video laryngoscopy. Under direct visualization, a cauliflower-like tumor mass was observed on the lingual surface of the epiglottis.
Figure 5. A 7.0-mm reinforced endotracheal tube was then advanced through the glottis.
3. Discussion
This case report details the airway management of a 69 - year - old male patient with a mass on the lingual surface of the epiglottis. In light of preoperative imaging studies, electronic nasopharyngolaryngoscopic findings, and clinical presentations, the objective of airway management was to avert airway obstruction by the mass following anesthesia and to prevent ventilation and intubation difficulties stemming from bleeding of the mass.
The selection of the anesthesia intubation approach for epiglottic masses should be predicated on the size and location of the masses, along with the patient's specific circumstances. Typically, there are the following options:
Firstly, when the anesthesiologist makes a choice, awake intubation guided by a nasotracheal fiberoptic bronchoscope can be considered
[6]
Kim S J, Lee H, Choi S Y, et al. Successful wire-guided fiberoptic nasotracheal intubation in a patient with hemifacial microsomia - A case report [J]. Anesth Pain Med (Seoul), 2020, 15(1): 73-77.
. If the tumor is not very large and the location permits, nasal awake intubation can be chosen
[7]
Ahmad I, El-Boghdadly K, Bhagrath R, et al. Difficult Airway Society guidelines for awake tracheal intubation (ATI) in adults [J]. Anaesthesia, 2020, 75(4): 509-528.
. This method can be carried out while the patient remains conscious, which is helpful for the doctor to observe the patient's reaction and breathing condition. However, there are risks such as nasal discomfort, nosebleeds, sinusitis, and nasal septum perforation during the intubation process. If the patient does not cooperate well, it will increase the risk of tumor bleeding. In addition, since awake intubation requires the patient to remain conscious, it may cause the patient to feel anxious or uncomfortable
[8]
Warwick E, Yoon S, Ahmad I. Awake Tracheal Intubation: An Update [J]. Int Anesthesiol Clin, 2024, 62(4): 59-71.
Secondly, when the anesthesiologist decides to perform a tracheotomy
[9]
Nielsen M K, Hägerström E G, Trolle W. [Tracheotomy] [J]. Ugeskr Laeger, 2017, 179(7).
[9]
. If the mass significantly compromises the airway, or in the presence of other complex factors or during emergencies, when the risk of tracheal intubation is prohibitively high or intubation has failed, tracheotomy may be warranted. In the case of this patient, although tracheotomy was the final step of the surgical procedure, performing tracheotomy prior to the commencement of the operation could potentially impact the key surgical steps and elevate the risk of infection
[10]
Grønhøj C, Charabi B, Buchwald C V, et al. Indications, risk of lower airway infection, and complications to pediatric tracheotomy: report from a tertiary referral center [J]. Acta Otolaryngol, 2017, 137(8): 868-871.
Jotic A D, Milovanovic J P, Trivic A S, et al. Predictors of Complications Occurrence Associated With Emergency Surgical Tracheotomy [J]. Otolaryngol Head Neck Surg, 2021, 164(2): 346-352.
. Additionally, conducting tracheotomy under local anesthesia may induce anxiety or discomfort in the patient, and in severe cases, give rise to psychological problems, thereby significantly influencing the patient's overall treatment experience. Nevertheless, tracheotomy can rapidly expose the airway for ventilation, thus rendering it a viable backup option.
Thirdly, when the anesthesiologist selects tracheal intubation using an oral electronic video laryngoscope
[12]
Cangiani L H, Vicensotti E, Ramos G C, et al. [Use of video laryngoscope for tracheal intu bation in patient with oral cavity mass: case report] [J]. Braz J Anesthesiol, 2020, 70(4): 434-439.
. This typically necessitates general anesthesia to mitigate the patient's discomfort and reactions
[13]
Wang L, Li H, Zhong Y, et al. Comparative Analysis of Hemodynamic Responses and Oropharyngeal Complications in Tracheal Intubation: Evaluating Conventional, Video, and Rigid Video Laryngoscopes Under General Anesthesia[J]. Med Sci Monit, 2024, 30: e944916.
. To avert airway collapse and blockage by the mass after the patient is anesthetized, it is essential to first assess the adequacy of the patient's ventilation while preserving spontaneous respiration before proceeding with tracheal intubation
[14]
Tang Z H, Chen Q, Huang W, et al. Difficult airway management in 25 hospitals across China: A multicenter cross-sectional study [J]. J Clin Anesth, 2025, 102: 111766.
. In the present case, the mass was situated on the lingual surface of the epiglottis. By using an electronic video laryngoscope to lift the epiglottis, the glottis could be exposed. With clear visualization, every effort should be exerted to avoid contact with the mass, thereby preventing mass bleeding. After the administration of analgesic and sedative medications, and upon confirmation of normal ventilation, a muscle relaxant was administered to the patient. Subsequently, the glottis was promptly exposed using an electronic video laryngoscope, and tracheal intubation was carried out with meticulous care.
In our case, there was no contact with the tumor throughout the intubation process and the tumor did not obstruct the airway. We ensured the safety of anesthesia throughout the entire operation while maximizing the patient's satisfaction with the medical experience.
4. Conclusion
Video laryngoscopy-assisted orotracheal intubation represents an optimal approach for securing the airway while preserving integrity of lingual epiglottic lesions, with minimal associated tissue trauma. However, successful and safe ventilation requires coordinated expertise from both experienced anesthesiologists and otolaryngology surgeons.
Author Contributions
Ying Su is the sole author. The author read and approved the final manuscript.
Conflicts of Interest
There have no conflict of interest.
References
[1]
Matsumoto T, Iwamoto T, Nakajima Y, et al. Evaluation of the Adequacy of Using the Supraglottic Airway Device (i-gel®) in Cases With Epiglottic Masses: A Mannequin Simulation Study [J]. Cureus, 2024, 16(11): e74734.
Varathan V, Mat Baki M, Kalimuthu S. A Case Report of an Unusual Presentation of Epiglottic Cyst Causing Airway Obstruction in an Adult [J]. Cureus, 2023, 15(3): e35863.
Zhang R, Jiang X, Feng J. Difficult endotracheal intubation due to a large epiglottic cyst: A case report [J]. Medicine (Baltimore), 2023, 102(24): e34026.
Takaishi K, Otsuka R, Fujiwara S J, et al. A Retrospective Case Series of Anesthetic Patients With Epiglottic Cysts [J]. Anesth Prog, 2021, 68(3): 168-177.
Kim S J, Lee H, Choi S Y, et al. Successful wire-guided fiberoptic nasotracheal intubation in a patient with hemifacial microsomia - A case report [J]. Anesth Pain Med (Seoul), 2020, 15(1): 73-77.
Ahmad I, El-Boghdadly K, Bhagrath R, et al. Difficult Airway Society guidelines for awake tracheal intubation (ATI) in adults [J]. Anaesthesia, 2020, 75(4): 509-528.
Nielsen M K, Hägerström E G, Trolle W. [Tracheotomy] [J]. Ugeskr Laeger, 2017, 179(7).
[10]
Grønhøj C, Charabi B, Buchwald C V, et al. Indications, risk of lower airway infection, and complications to pediatric tracheotomy: report from a tertiary referral center [J]. Acta Otolaryngol, 2017, 137(8): 868-871.
Jotic A D, Milovanovic J P, Trivic A S, et al. Predictors of Complications Occurrence Associated With Emergency Surgical Tracheotomy [J]. Otolaryngol Head Neck Surg, 2021, 164(2): 346-352.
Cangiani L H, Vicensotti E, Ramos G C, et al. [Use of video laryngoscope for tracheal intu bation in patient with oral cavity mass: case report] [J]. Braz J Anesthesiol, 2020, 70(4): 434-439.
Wang L, Li H, Zhong Y, et al. Comparative Analysis of Hemodynamic Responses and Oropharyngeal Complications in Tracheal Intubation: Evaluating Conventional, Video, and Rigid Video Laryngoscopes Under General Anesthesia[J]. Med Sci Monit, 2024, 30: e944916.
Tang Z H, Chen Q, Huang W, et al. Difficult airway management in 25 hospitals across China: A multicenter cross-sectional study [J]. J Clin Anesth, 2025, 102: 111766.
Ying, S. (2025). Difficult Endotracheal Intubation Due to an Epiglottic Mass: A Case Report. International Journal of Anesthesia and Clinical Medicine, 13(2), 89-92. https://doi.org/10.11648/j.ijacm.20251302.15
Ying, S. Difficult Endotracheal Intubation Due to an Epiglottic Mass: A Case Report. Int. J. Anesth. Clin. Med.2025, 13(2), 89-92. doi: 10.11648/j.ijacm.20251302.15
Ying S. Difficult Endotracheal Intubation Due to an Epiglottic Mass: A Case Report. Int J Anesth Clin Med. 2025;13(2):89-92. doi: 10.11648/j.ijacm.20251302.15
@article{10.11648/j.ijacm.20251302.15,
author = {Su Ying},
title = {Difficult Endotracheal Intubation Due to an Epiglottic Mass: A Case Report
},
journal = {International Journal of Anesthesia and Clinical Medicine},
volume = {13},
number = {2},
pages = {89-92},
doi = {10.11648/j.ijacm.20251302.15},
url = {https://doi.org/10.11648/j.ijacm.20251302.15},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijacm.20251302.15},
abstract = {Epiglottic masses may present as cystic, infectious, neoplastic, or systemic disease manifestations. Their size and location can lead to airway obstruction, increasing the difficulty of general anesthesia induction. Perioperative management for such patients requires meticulous planning to prevent sudden airway challenges post-anesthesia. Multidisciplinary collaboration (anesthesiology and otolaryngology) and the use of visualization devices (e.g., video laryngoscopy) are critical for ensuring airway safety. We described the anesthesia management for a 69-year-old male with a glottic mass. Laryngoscopy and CT revealed a 2.7×2.0 cm cauliflower-like mass on the lingual surface of the epiglottis (squamous high-grade intraepithelial neoplasia/carcinoma in situ). After comprehensive evaluation of the airway and perioperative drug interactions, appropriate sedatives, analgesics, and muscle relaxants were selected. The patient successfully completed the surgery and was discharged. The selection of the anesthesia intubation approach for epiglottic masses should be predicated on the size and location of the masses, along with the patient's specific circumstances. This case underscores the significance that conducting a thorough preoperative assessment of the patient prior to surgery and implementing multidisciplinary cooperation in light of the patient's condition can substantially mitigate anesthesia - related risks. Video laryngoscopy-assisted endotracheal intubation is the preferred method for protecting lingual epiglottic masses, minimizing tumor injury risks. However, its successful and safe implementation requires collaboration between experienced anesthesiology and otolaryngology teams.},
year = {2025}
}
TY - JOUR
T1 - Difficult Endotracheal Intubation Due to an Epiglottic Mass: A Case Report
AU - Su Ying
Y1 - 2025/08/18
PY - 2025
N1 - https://doi.org/10.11648/j.ijacm.20251302.15
DO - 10.11648/j.ijacm.20251302.15
T2 - International Journal of Anesthesia and Clinical Medicine
JF - International Journal of Anesthesia and Clinical Medicine
JO - International Journal of Anesthesia and Clinical Medicine
SP - 89
EP - 92
PB - Science Publishing Group
SN - 2997-2698
UR - https://doi.org/10.11648/j.ijacm.20251302.15
AB - Epiglottic masses may present as cystic, infectious, neoplastic, or systemic disease manifestations. Their size and location can lead to airway obstruction, increasing the difficulty of general anesthesia induction. Perioperative management for such patients requires meticulous planning to prevent sudden airway challenges post-anesthesia. Multidisciplinary collaboration (anesthesiology and otolaryngology) and the use of visualization devices (e.g., video laryngoscopy) are critical for ensuring airway safety. We described the anesthesia management for a 69-year-old male with a glottic mass. Laryngoscopy and CT revealed a 2.7×2.0 cm cauliflower-like mass on the lingual surface of the epiglottis (squamous high-grade intraepithelial neoplasia/carcinoma in situ). After comprehensive evaluation of the airway and perioperative drug interactions, appropriate sedatives, analgesics, and muscle relaxants were selected. The patient successfully completed the surgery and was discharged. The selection of the anesthesia intubation approach for epiglottic masses should be predicated on the size and location of the masses, along with the patient's specific circumstances. This case underscores the significance that conducting a thorough preoperative assessment of the patient prior to surgery and implementing multidisciplinary cooperation in light of the patient's condition can substantially mitigate anesthesia - related risks. Video laryngoscopy-assisted endotracheal intubation is the preferred method for protecting lingual epiglottic masses, minimizing tumor injury risks. However, its successful and safe implementation requires collaboration between experienced anesthesiology and otolaryngology teams.
VL - 13
IS - 2
ER -
Ying, S. (2025). Difficult Endotracheal Intubation Due to an Epiglottic Mass: A Case Report. International Journal of Anesthesia and Clinical Medicine, 13(2), 89-92. https://doi.org/10.11648/j.ijacm.20251302.15
Ying, S. Difficult Endotracheal Intubation Due to an Epiglottic Mass: A Case Report. Int. J. Anesth. Clin. Med.2025, 13(2), 89-92. doi: 10.11648/j.ijacm.20251302.15
Ying S. Difficult Endotracheal Intubation Due to an Epiglottic Mass: A Case Report. Int J Anesth Clin Med. 2025;13(2):89-92. doi: 10.11648/j.ijacm.20251302.15
@article{10.11648/j.ijacm.20251302.15,
author = {Su Ying},
title = {Difficult Endotracheal Intubation Due to an Epiglottic Mass: A Case Report
},
journal = {International Journal of Anesthesia and Clinical Medicine},
volume = {13},
number = {2},
pages = {89-92},
doi = {10.11648/j.ijacm.20251302.15},
url = {https://doi.org/10.11648/j.ijacm.20251302.15},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijacm.20251302.15},
abstract = {Epiglottic masses may present as cystic, infectious, neoplastic, or systemic disease manifestations. Their size and location can lead to airway obstruction, increasing the difficulty of general anesthesia induction. Perioperative management for such patients requires meticulous planning to prevent sudden airway challenges post-anesthesia. Multidisciplinary collaboration (anesthesiology and otolaryngology) and the use of visualization devices (e.g., video laryngoscopy) are critical for ensuring airway safety. We described the anesthesia management for a 69-year-old male with a glottic mass. Laryngoscopy and CT revealed a 2.7×2.0 cm cauliflower-like mass on the lingual surface of the epiglottis (squamous high-grade intraepithelial neoplasia/carcinoma in situ). After comprehensive evaluation of the airway and perioperative drug interactions, appropriate sedatives, analgesics, and muscle relaxants were selected. The patient successfully completed the surgery and was discharged. The selection of the anesthesia intubation approach for epiglottic masses should be predicated on the size and location of the masses, along with the patient's specific circumstances. This case underscores the significance that conducting a thorough preoperative assessment of the patient prior to surgery and implementing multidisciplinary cooperation in light of the patient's condition can substantially mitigate anesthesia - related risks. Video laryngoscopy-assisted endotracheal intubation is the preferred method for protecting lingual epiglottic masses, minimizing tumor injury risks. However, its successful and safe implementation requires collaboration between experienced anesthesiology and otolaryngology teams.},
year = {2025}
}
TY - JOUR
T1 - Difficult Endotracheal Intubation Due to an Epiglottic Mass: A Case Report
AU - Su Ying
Y1 - 2025/08/18
PY - 2025
N1 - https://doi.org/10.11648/j.ijacm.20251302.15
DO - 10.11648/j.ijacm.20251302.15
T2 - International Journal of Anesthesia and Clinical Medicine
JF - International Journal of Anesthesia and Clinical Medicine
JO - International Journal of Anesthesia and Clinical Medicine
SP - 89
EP - 92
PB - Science Publishing Group
SN - 2997-2698
UR - https://doi.org/10.11648/j.ijacm.20251302.15
AB - Epiglottic masses may present as cystic, infectious, neoplastic, or systemic disease manifestations. Their size and location can lead to airway obstruction, increasing the difficulty of general anesthesia induction. Perioperative management for such patients requires meticulous planning to prevent sudden airway challenges post-anesthesia. Multidisciplinary collaboration (anesthesiology and otolaryngology) and the use of visualization devices (e.g., video laryngoscopy) are critical for ensuring airway safety. We described the anesthesia management for a 69-year-old male with a glottic mass. Laryngoscopy and CT revealed a 2.7×2.0 cm cauliflower-like mass on the lingual surface of the epiglottis (squamous high-grade intraepithelial neoplasia/carcinoma in situ). After comprehensive evaluation of the airway and perioperative drug interactions, appropriate sedatives, analgesics, and muscle relaxants were selected. The patient successfully completed the surgery and was discharged. The selection of the anesthesia intubation approach for epiglottic masses should be predicated on the size and location of the masses, along with the patient's specific circumstances. This case underscores the significance that conducting a thorough preoperative assessment of the patient prior to surgery and implementing multidisciplinary cooperation in light of the patient's condition can substantially mitigate anesthesia - related risks. Video laryngoscopy-assisted endotracheal intubation is the preferred method for protecting lingual epiglottic masses, minimizing tumor injury risks. However, its successful and safe implementation requires collaboration between experienced anesthesiology and otolaryngology teams.
VL - 13
IS - 2
ER -